Cerebellar cavernous hemangiomas (also called cavernomas or cavernous malformations) are low-flow vascular lesions in the brain that can cause symptoms due to bleeding or compression.
What is a cerebellar cavernous hemangioma?
– A cavernous hemangioma is a cluster of dilated capillaries with no intervening brain tissue.
– In the cerebellum, these lesions can cause coordination issues, dizziness, and headaches—especially if they bleed.
– They are angiographically occult (not seen on angiogram) but very clear on MRI.
Patient Presentation:
Depends on location, size, and presence of hemorrhage.
Common Symptoms:
– Headache
– Dizziness or vertigo
– Ataxia (gait imbalance)
– Nausea, vomiting
– Signs of increased intracranial pressure (if large or bleeding)In some cases, they’re found incidentally on imaging.
Imaging Findings:
MRI—Gold standard
– “Popcorn” or “mulberry” appearance with a mixed-signal core (due to blood at different stages).
– Surrounded by a hypointense hemosiderin rim (from previous microbleeds).
Best seen on:
– T2-weighted images
– Gradient Echo (GRE) or SWI for blooming artifact from hemosiderin.
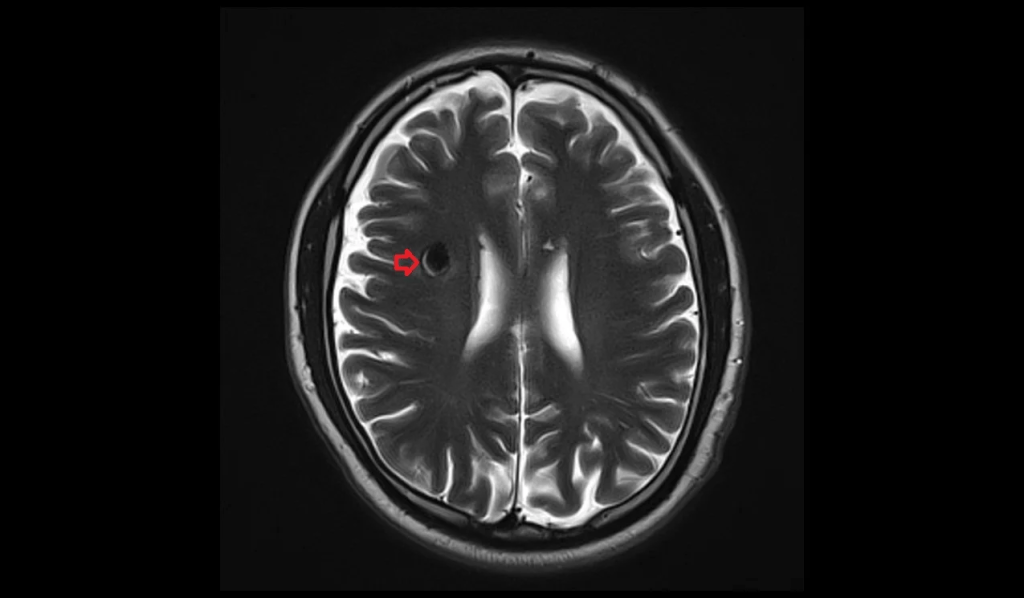

T2 axial images show cavernoma
Angiography:
The results are typically negative, as these are low-flow lesions .
Surgical Indications
Surgery is considered if:
– Recurrent bleeding
– Symptomatic lesion (e.g., ataxia, pressure symptoms)
– Accessible cerebellar location
Asymptomatic lesions are usually observed, unless they are high-risk (e.g., close to the fourth ventricle or brainstem).
Surgical Approach
Suboccipital Craniotomy
Most common approach for midline or paramedian cerebellar cavernomas.
Steps:
1. The patient is placed in a prone or park bench position.
2. Midline posterior fossa incision with suboccipital bone removal.
3. Dura is opened, and the cerebellar cortex is gently retracted .
4. Lesion is carefully dissected and removed; it may have surrounding gliosis or hemosiderin.
5. Hemostasis and closure.Key Point: Avoid incomplete resection, as residual tissue can bleed again.
Postoperative Considerations
– Monitor for hydrocephalus (especially if lesion near 4th ventricle).
– Neurological exam for cerebellar signs
– Repeat MRI to confirm gross total resection
– Seizure prophylaxis (rarely needed unless supratentorial)
Brainstem Cavernous Malformation Surgery:
Posterior Petrosectomy for Resection of Pontine Cavernous Malformation:
Every case is a classroom. Each incision serves as a lesson. Observing from the sidelines today, I witnessed not just a procedure but a performance of precision, patience, and purpose.
Here’s to many more steps into the OR, and many more pages in my journey as a student of the brain.

Leave a comment